




Human activity in this place seems to have completely died out; the streets are empty and deserted and all the houses are left desolate. Those who were not struck by the plague in the town itself fled terror-stricken and were overtaken by the black epidemic outside the town. The bazaars and markets are closed. Dogs alone roam in the streets, howling and feeding on the corpses of their former masters. The stench is horrible. The hospitals are abandoned. There are no ill people anymore and no medical men—all have died. Only on a few beds lie the dead bodies of those who expired last.
This is not a passage from Boccaccio’s Decameron, the first-hand account of the Black Death of the 14th century, but a dispatch from northeast China published in the British medical journal The Lancet in 1911. It described the dire situation in the region of China then called Manchuria caused by the last great epidemic of plague the world has yet known. In less than a year, between 40,000 and 60,000 people died. Mortality, The Lancet’s correspondent reported, was one hundred percent. You got it, you died. Manchuria in 1910, when this plague broke out on the border between Mongolia and China along the Heilong river, was on the periphery of the crumbling Chinese Qing empire and the site of global geopolitical conflict involving Japan, Russia, and the Western Great Powers, as well as China. China’s response to the outbreak set the stage for much of the country’s public health development in the ensuing century.
As the world continues to reel from the COVID-19 pandemic, the onslaught of new developments, disrupted routines, and fast-evolving medical research and advice trap us in a kind of eternal present. Each day feels unprecedented. But as we struggle to formulate responses and plans for current challenges, the history of disease outbreaks and how they came to an end still deserves attention. The geopolitical aspects of past epidemics are of course conditioned by specific cultures and historical circumstances. But, at least since the Black Death, the macrohistories of disease have followed a tediously similar course. Over the past six centuries, in different places, with different diseases, and with different political systems, epidemics have tended to play out in a strikingly similar and sadly tragic way.
For several decades, I have studied and taught about global epidemics, and in medical writings, contemporary accounts, as well as fiction, certain constant themes emerge: 1) early suspicions of trouble are suppressed as alarmist; 2) social authorities such as government, business, and religious leaders conceal the problem as destabilizing society; 3) responses eventually occur because of popular pressure; 4) scapegoating is almost always present; and 5) economic, social, and geopolitical factors outweigh medical and scientific factors. Epidemics challenge political systems, and conversely, are used by political systems for both internal and external goals. This has been especially true for China, where the tradition linking public welfare to political legitimacy is particularly strong. The Great Manchurian Plague of 1910-1911, Mao’s Snail Fever campaign in the late 1950s and early 1960s, and the SARS outbreak in 2003 provide three clear examples of China’s responses to the challenges of epidemic disease. Sadly, common and seemingly timeless themes emerge.
Plague, the infection by the bacterium called Yersinia pestis, originated in Central Asia by several complicated evolutionary steps approximately 20,000 years ago, and because of the complicated ecology of humans, fleas, and other animals, especially rodents, plague has periodically ravaged human populations since then.
As we have come to appreciate more fully in recent years, humans and animals exist in a single disease ecosystem, with germs passed between species much more than we previously thought. This “One Health” concept now recognizes this ecological approach to disease, understanding, for example, the role habitat changes have in changing the interaction of wild species, domestic animals, and human beings in ways that spread novel infections agents, most recently COVID-19. The Manchurian plague had its origin in endemic infection of Siberian marmots of Central Asia, long a source of local outbreaks of plague. The marmot, a rodent host of the plague germ, was hunted for food and fur for centuries, and local marmot hunters had evolved hunting practices to avoid contact with sick marmots. Two events changed the equilibrium of this human-animal interaction in Central Asia in the first years of the 20th century: the world-wide market for marmot fur greatly expanded due to the discovery by German chemists of ways to dye cheap marmot fur to resemble expensive sable, and the completion of the new railroad lines in northern China allowing rapid, cheap access to the marmot-hunting regions of Manchuria and Mongolia. Itinerant hunters from Shandong province, across the Bohai Sea, flooded the plains of north China, living in temporary camps. According to Chinese investigators who described the start of the outbreak in the “Report of the International Plague Conference,” held in Shenyang (Mukden) in 1911, these hunters did not know the traditional ways to avoid sick marmots, and indeed, found it easier to catch sick animals than healthy ones. Although local plague outbreaks in Central Asia had been linked to sick marmots since the mid-19th century, the doctors investigating the Manchurian Plague in 1910 had the recent knowledge, from Dr. Paul-Louis Simond in Karachi, that fleas could act as a vector between animals and humans, and deduced that these hunters became infected with plague via bites from fleas that lived on the marmots’ bodies. As the marmot season of 1910 came to a close on the frozen plains of northern China, they boarded the new trains and headed home for the Lunar New Year reunions of early 1911. Sickness and death tracked the railroads through Manchuria from late 1910 until early spring 1911.
In 1910, the three northeast provinces of China were nominally under the administrative control of a viceroy, Xiliang. The Qing court was struggling with revolutionary challenges in the south and welcomed the opportunity to ignore Manchuria. But the viceroy, and indeed, China, was only nominally in control. As a result of the agreements following the 1905 Russo-Japanese war, Japan and Russia exerted de facto control of much of Manchuria. Both countries saw the devastation of the plague as an opportunity to gain hegemony in north China. Control of the railways was paramount, together with control of agricultural and mining resources. Much of the Russian response to the plague, especially in the then Russian city of Harbin, was directed by Russian military personnel; in the south, in the Japanese city of Dalian, it was the South Manchuria Railway Company that was in control. Response to the epidemic was almost totally decentralized and left to the local leaders, both Chinese and foreign, who often had competing agendas. The larger cities had committees of the foreign consuls, which exerted considerable sway over the local Chinese officials. Their goal was to tamp down the local Chinese population’s fears of quarantine while maintaining trade and business for the foreign interests. Because of the principle of “extraterritoriality,” whereby foreign powers asserted their home country’s authority and laws over their citizens and neighborhoods in China, these foreign consular committees often exerted more real control than the weak local Chinese representatives of the Qing court.
As seen in contemporary newspaper accounts and photos, as well as reports to the International Plague Conference in Shenyang, quarantine was particularly brutal and often lethal in some places. The infected marmot hunters traveled by train, so in Harbin, for example, Russian authorities ordered box cars full of people simply pulled off on sidings and left for several days to see if anyone died. If not, the occupants were released. If a death occurred, quarantine was continued until all had died, or until the deaths stopped. Needless to say, escapes were frequent and disease maps published in the “Report of the International Plague Conference” show that stopping the railway cars often resulted in diversion of disease into the countryside. Contemporary records show that posters to inform the public were inflammatory and often deliberately misleading. Public posters showed piles of skulls and other scary icons representing disease being doused with disinfectant, as well as images of soldiers attacking the poor to enforce public health measures. Because of the low level of popular literacy, posters seemed to rely on imagery to convey the desired message.
The Qing government provided minimal support and less interference. The viceroy was freed from Imperial bureaucracy, both by distance and financial independence, to craft his own responses with the aid of two unusual young helpers, an unknown but talented physician, Wu Lien-teh, and an American-educated Chinese diplomat, Sao-Ke Alfred Sze. Wu, a 31-year-old Chinese Malaysian who had recently graduated from the University of Cambridge and spent time in Europe with leading bacteriologists, was working in northern China in part because, as a non-European, he sensed the unlikelihood of securing a permanent research position in his native British Malaya. His actions in bringing modern medicine to this epidemic, his talent for negotiating between the consular committees and the local Qing officials, and his personal diplomacy and leadership have become the stuff of legend. For example, young Wu had to contend with the pompous Baron Kitasato Shibasaburō, at the time acknowledged as co-discoverer of the plague bacillus, who threatened to disrupt the conference if he did not head it. Wu quietly supplied the American researcher Robert P. Strong with access to much important experimental material before the congress so that Strong and Wu would be able to counter Kitasato’s bluster with their most recent findings. To mollify Kitasato, Wu made a big fuss over getting Kitasato appointed chair of what Wu billed as the most key part of the meeting. Wu pushed for actions based on the best medical knowledge, such as isolation and quarantine, cremation of the dead, meticulous post-mortem examinations, and laboratory inoculation studies. With those actions, together with the winter interruption of the marmot hunting season, and the draconian quarantine measures taken out of fear, the epidemic ended in early spring 1911. It was Wu’s firm hand and the immediate responses of the epidemic to his measures that forestalled Japan’s plan to send military personnel to “protect” Manchuria as well as the Russian plan to take over the railway cities in north China. Wu managed to convert the pressure for military intervention into China’s organization of the international scientific conference to deal with the plague. The proceedings of this conference remain the most authoritative source of scientific studies on a bubonic plague epidemic that we have.
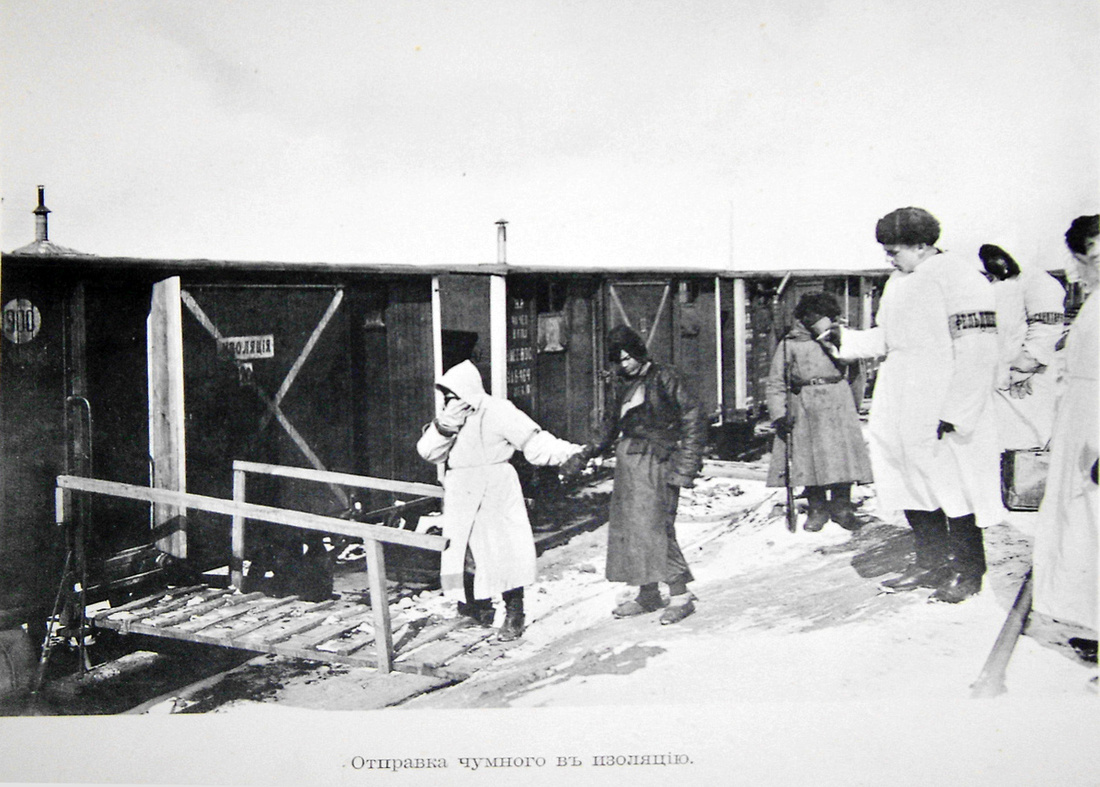
Quarantined railway cars during the 1910-1911 plague outbreak in Manchuria, near Harbin.
Wu went on to set up the North Manchurian Plague Prevention Service, an organization that eventually evolved into the public health service for the whole of China. Public health in China borrowed from Western modes out of medical necessity and there are still vestiges of this origin, but political considerations, in which failures are attributed to ideological weakness and hence have drastic consequences, as well as cover-ups and data manipulation, have been all too common in recent times.
With the founding of the People’s Republic of China in 1949, it is no surprise that providing health services to the masses would be a priority for the new government of Mao Zedong. With infectious diseases prevalent, life-expectancy low, and physicians few, the new government decided to attack the common, troublesome endemic parasitic disease known to many Chinese as Snail Fever (schistosomiasis). The choice of Snail Fever as the target of one of the first mass-mobilization campaigns of the new government was an example of what historian Miriam Gross has described as the “dressing up [of] politically driven public policy in a scientific guise.” Other endemic diseases were equally problematic, but Snail Fever was visible, the enemy (water snails) was easily identified, and the campaign would serve as a public education in science and scientific socialism.
The tension between the mass-mobilization campaign and increasing scientific knowledge of parasitology and public health was present from the start. The advice officials dispensed to the Chinese public was more propaganda than science, emphasizing progress, communism and national pride, and economic advantages. The campaign, as has been documented recently by Gross, was more an experiment in mass education and indoctrination techniques than in public health promotion. As Gross summarized, “Few parts of the snail fever campaign were more important than disseminating scientific knowledge and attitudes to the masses.” The Party’s plan included merging the people with science and technology, strengthening the people in order to progress; scientific transformation of the masses was a key goal of Chairman Mao. After nearly two decades of effort, results were still spotty and international evaluation suggested the campaign had been a failure, assuming its real goal was to eradicate or even control Snail Fever. Comparing the Chinese Snail Fever campaign to the WHO’s global anti-malaria campaign that started in 1955, Gross observes: “A final regrettable similarity between the campaigns was their refusal to learn from mistakes despite decades of time and multiple campaign peaks.” Politics trumped science, again.
The 2003 outbreak of the Severe Acute Respiratory Syndrome (SARS) in China provides a more recent example where, again, health took a back seat to economics, politics, and “stability.” Early cases appeared in late 2002 in Guangdong province and have been traced to a species of bats, with civets as the intermediate host, a good example of the One Health concept. As has been well-documented, China’s fragmented health system was slow to respond, and in some cases deliberate obfuscation was present. Interactions with global health surveillance organizations were also compromised until exposed by a few courageous Chinese physicians and international journalists. Such politically driven actions delayed identification of the viral agent and allowed its spread to other regions in Southeast Asia, and eventually other parts of the world. Fortunately, quarantine and surveillance measures introduced around the world resulted in containment of the epidemic by July 2003.
Reliable information, no matter how unwelcome, understanding and acceptance of the significance of that information, actions directed by the best scientific knowledge, and recognition and resistance to economic and political pressures are the four themes that emerge as desiderata for management of public health crises. One or more of these key responses was lacking in these challenges to China as well as in many (if not most) such challenges in the past several centuries. Epidemics have uses; they have been used as pretexts for scapegoating, mass mobilizations, military actions, and social control. They have also been opportunities for important advances in scientific and medical knowledge, and yes, the arts, too. Like wars and revolutions, epidemics are major stressors on human cultures and they deserve historians’ attention every bit as much. Culture-specific responses to the challenge of an epidemic can lay bare features of a society just as surely as other major disruptions. The abrupt outbreak of plague in Manchuria, the chronic endemic problem of Snail Fever in China, and the short but lethal epidemic of SARS starting in Guangdong province all share common responses although occurring over the course of slightly more than a century. The most noteworthy, relevant, and frustrating of these responses that they have in common with the current COVID-19 outbreak is the uncertainty of early information about the start of the epidemic. The urge to ignore early cases, to suppress information, to deny and denigrate messengers of bad news, and to prevent full investigation all are features of the current epidemic that certainly have harmful consequences in the long run. Historical analyses suggest that selective changes in just a few of these actions might be highly effective in dealing with epidemic disease. Information is power, but power for whom?